2 minute read
Dementia remains a leading cause of disability and death in the UK, accounting for more years lived with disability than any other condition (Palliative and end of life care profiles January 2025 update: statistical commentary – GOV.UK). In Kirklees, the number of people aged 65+ living with dementia is projected to rise from approximately 5,986 in 2025 to 8,192 by 2040 (Projecting Older People Population Information System), a 37% increase over 15 years. As of April 2025, 65.5% of people aged 65+ estimated to have dementia in England had a formal diagnosis. This trend reflects national projections, with the UK total expected to reach 1.4 million by 2040 (Dementia Statistics Hub | Alzheimer’s Research UK).
Dementia is responsible for 8% of deaths in men and 11% in women aged 65+. It affects 1 in 14 people over 65 and 1 in 5 over 80. Women are disproportionately affected, comprising 57% of the 982,000 people living with dementia in the UK.
As of January 2025, 34,033 people in England (6.9% of those diagnosed) were diagnosed with dementia before age 65. The estimated prevalence for young onset dementia (diagnosed between ages 30–64) is 92 per 100,000. The average time to diagnosis for younger people is 4.4 years, compared to 2.2 years for those over 65 (Young onset dementia facts and figures – Young Dementia Network). In Kirklees, approximately 120 individuals are estimated to be living with young onset dementia (Primary Care Dementia Data, January 2025 – NHS England Digital).
People from Black African-Caribbean and South Asian backgrounds are at higher risk of developing dementia and are more likely to experience delayed diagnosis and reduced access to services, yet these groups are often underrepresented in diagnosis and care pathways (Dementia and BAME Communities – Race Equality Foundation). Cultural stigma, language barriers, and lack of culturally competent services contribute to disparities (Challenges of Dementia Care for Ethnic Minorities in the UK). Individuals with learning disabilities, particularly those with Down’s Syndrome, are four times more likely to develop dementia at an earlier age.
Age is the primary risk factor, but others include genetics, cardiovascular health, and lifestyle choices. Positive behaviours, such as a healthy diet, physical activity, not smoking, and reduced alcohol intake can lower risk.
Figure 1: Factors linked to dementia risk
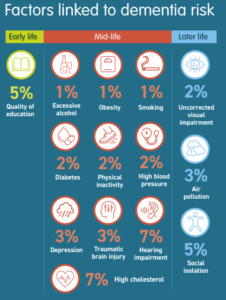
From Kirklees Council leaflet: Reducing your risk of developing dementia
Many people living with dementia continue to live in the community, primarily cared for by unpaid carers. The Kirklees Dementia Hub offers vital support and information and advice services across Kirklees.
About the issue
Dementia is a significant health issue, accounting for more years of disability than any other condition.
With an estimated 982,000 people living with dementia in the UK, Alzheimer’s Research UK report that the number of people living with dementia is predicted to rise to 1.4 million by 2040. Dementia currently represents one of the greatest challenges to our health and social care landscape. With no known cure and with limited treatments available, dementia is redefining our individual and collective experience of ageing, irrevocably changing the lives of citizens and their families across Kirklees (Diagnosis of dementia – Dementia Statistics Hub (ARUK)).
The term ‘dementia’ is used to describe a set of symptoms which cause the ongoing decline of the brain. Dementia is progressive, meaning symptoms will get worse over time. As their remaining strengths begin to erode, people will experience a variety of symptoms of dementia, which may include a decline of functions such as memory, processing skills, orientation, understanding, judgement, calculation, learning, language, wayfinding and more, which will begin to affect a person’s everyday tasks (Dementia information – Alzheimer’s Research UK).
There are several diseases that cause dementia. Alzheimer’s disease is the most common form, accounting for around 60% of all cases, followed by cerebrovascular disease (vascular dementia), and dementia with Lewy bodies which together account for 15-20% of cases. In young-onset dementia (under 65yrs), frontal-temporal dementia is the most common disease, followed by Alzheimer’s. The rarer forms of dementia are more likely in the under 65 age group and account for some of the more challenging behaviours. Less common diseases that may also cause dementia include Parkinson’s Disease, Huntington’s Disease, HIV and AIDS, Korsakoff’s Syndrome, Creutzfeldt-Jakob Disease, Multiple Sclerosis and Motor Neurone Disease amongst others. People may also have a combination of dementias such as Alzheimer’s and Dementia with Lewy Bodies, the term for this is ‘mixed dementia’.
There are a number of potential pharmacological (e.g., antipsychotic drugs), and non-pharmacological (e.g., cognitive behavioural therapy) interventions that focus on treating the symptoms of some dementias, but they are not suitable for everyone. Nevertheless, people with dementia are at an increased risk of physical health problems and become increasingly dependent on health and social care services and on other people, i.e., friends and family, as there is a progressive decline in multiple areas of brain function, including memory, reasoning, communication skills and the ability to carry out daily activities. There are individual differences in the type, speed and progression of dementia. Each person is unique and will experience symptoms differently (Dementia information – Alzheimer’s Research UK).
Dementia is not restricted to age, gender or ethnicity and impacts individuals from all walks of life and communities. However, there are notable disparities in the risk, occurrence, diagnosis, and management of dementia. People living with dementia are also at greater risk of social isolation, particularly as the condition begins to erode their existing strengths.
What significant factors are affecting this issue?
Increasingly, age is the main risk factor and an increase in the population aged over 65 years, particularly those aged over 85 years, is likely to lead to an increase in the numbers of people with dementia. Other factors include genetic background, medical history and health behaviours. About half of all cases of dementia have a vascular component (i.e. linked to the blood supply to the brain) and so are linked to smoking, diet and physical activity (Dementia information – Alzheimer’s Research UK).
Risk of dementia may be reduced by adopting positive health behaviours and raising awareness of these risk factors is a local priority.
Good nutrition contributes to healthy brain development, which may protect against the onset of dementia in later life. Obesity in midlife and diets rich in saturated fat, which predispose to cardiovascular disease, may increase the risk of developing dementia in later life. Maintaining an adequate diet is challenging for people with dementia, leading to a particularly high prevalence of under nutrition, people with dementia may take longer to eat, require prompting and encouragement and may have problems with co-ordination, swallowing and distraction from a noisy or over stimulating environment.
Up to half of all people with dementia also have depression. People with both dementia and depression have higher rates of disability and high rates of hospital admission. Around 40% of those aged 65 or over thought to be living with dementia do not have a diagnosis (Diagnosis of dementia – Dementia Statistics Hub (ARUK)).
National and Regional Picture
Nationally, approximately 982,000 people are estimated to be living with dementia, with 1 in 14 people over the age of 65 years and 1 in 5 people aged over 80 years affected by dementia. However, approximately only 1 in 3 people with dementia ever receive a formal diagnosis or have contact with specialist services (Prevalence and incidence – Dementia Statistics Hub).
Approximately 57% of the 982,000 people living with dementia in the UK are women, who are bearing a disproportional impact and are more likely to develop dementia than men. Locally, we can see variances between women and men, particularly in the older age groups. This is likely due to the longer life expectancy of women than men. However, women live longer in ill health or with a disability than men. In addition, women are more likely to become a carer for someone with dementia. By the age of 60, 1 in 5 women will have provided unpaid care to an elderly friend or relative (Dementia diagnosis and prevalence by Integrated Care Board).
An estimated 70,800 people living with dementia in the UK are living with young onset dementia, where symptoms occurred under the age of 65 (Young onset dementia: facts and figures – Dementia UK). Locally, around 120 individuals have younger onset dementia (under 65 years old). The average time to diagnosis is 4.4 years in younger people compared to 2.2 years for people aged over 65. In England in August 2018, the estimated dementia diagnosis rate for under 65s was 41%, compared to 68% for people aged over 65.
Prevalence rates for young onset dementia in minority ethnic communities are higher than for the population as a whole. People from these backgrounds are also less likely to receive a diagnosis or support (Dementia and BAME Communities – Race Equality Foundation).
Individuals with learning disabilities are at higher risk of developing dementia and the specific association between Down’s Syndrome and Alzheimer’s disease is well recognised. The assessment of cognitive impairment in learning disability needs special care, paying attention particularly to co-morbid physical and mental health disorders and less reliance of standard tests of cognition. People with Down’s Syndrome are four times more likely to develop dementia and for it to begin at an earlier age (Dementia in Down’s syndrome – Alzheimer’s Research UK). Locally, a learning disability and dementia pathway is in place and early discussions are being held to scope out a specific dementia screening programme for individuals over the age of 50 with Down’s Syndrome.
Regionally, the estimated number of people living with dementia in West Yorkshire is over 28,000, this is higher than the national (Integrated Care Board, ICB) average of 17,634. The number of people living with a diagnosis of dementia is 19,749, which is higher than the national ICB average of 11,563. In addition, 70% of people predicted to have dementia are known to services (Dementia diagnosis and prevalence by Integrated Care Board).
The Kirklees Picture
Locally, prevalence shows that approximately 5,968 out of 78,400 (ONS data) people aged over the age of 65 had dementia as at April 2025, and this figure is projected to rise to nearly 8,192 (Projecting Older People Population Information System, POPPI) by 2040. This is a 37% rise in over just 15 years. In addition, we know that there are around 120 people locally with dementia aged under 65 years and this number is expected to remain fairly stable until 2040 (Projecting Adult Needs and Service Information System, PANSI, and local case file records).
Table 1 : Projected change in number of people with dementia by age group
| Age group | 2025 | 2040 | % change |
| 30-64 | 120 | 114 | -5% |
| 65-69 | 389 | 426 | +10% |
| 70-74 | 607 | 784 | +29% |
| 75-79 | 1,152 | 1,306 | +13% |
| 80-84 | 1,330 | 1,760 | +32% |
| 85-89 | 1,301 | 1,796 | +38% |
| 90+ | 1,191 | 2,121 | +78% |
Source: POPPI and PANSI tools
This increase will likely place mounting pressure on already stretched health and social care services, intensify demand for specialist residential, domiciliary care, day care, respite care and significantly increase reliance on unpaid carers. The actual number of people who have a recorded diagnosis in Kirklees is approximately 3,300 (Kirklees Primary Care Data). This shows that although more than half of people predicted to have dementia are known to services, there is still a significant gap between this number and the number predicted to have dementia locally.
The Kirklees dementia prevention leaflet explains the small changes we can all do to reduce the risk of developing dementia.
Dying with Dementia
Dementia and Alzheimer’s Disease accounted for 12% of deaths registered in England and Wales in 2024 (Deaths due to dementia – Dementia Statistics Hub). The majority (56.4%) of deaths with a mention of dementia occurred in care homes (Statistical commentary: dementia profile, December 2024 update – GOV.UK). By comparison, a much lower proportion (25%) of all deaths in the general population aged 65+ happen in a care home setting.
People living with dementia are less likely to die at home than people dying with cancer, circulatory or respiratory diseases (Statistical commentary: dementia profile, December 2024 update – GOV.UK). Only 26.3% of people aged 65+ who died with a mention of dementia died in hospital, a significantly lower proportion than in the general population, where 43.4% of all deaths occurred in hospital in 2022 (Statistical commentary: dementia profile, December 2024 update – GOV.UK).
Dementia remains the leading cause of death for women in the UK. In 2023, over 48,000 women died with dementia, compared to 27,000 men (Death registration summary statistics, England and Wales – Office for National Statistics).
Only 1% of deaths with dementia occur in a hospice setting, compared with 4.7% of deaths in the general population aged 65+. People with dementia are less likely to die in a hospice than people dying of cancer (Palliative and end of life care profile December 2023 update: Statistical commentary – GOV.UK). In addition, people who die with dementia are more likely to die younger if they reside in more deprived areas. The proportion difference is small but significant and is more pronounced for people with vascular dementia (Dying with Dementia: briefing).
In 2023, only 15.5% of people aged 65+ who died with dementia did so at home, compared to 21% of the general population aged 65+. Nationally, 56% of people say they would prefer to die at home (Marie Curie report: Public attitudes to death, dying and bereavement in the UK re-visited: 2023 survey).
People living with dementia should have the opportunity to discuss advance care plans at every opportunity. Planning for end of life is important for anyone with a life-limiting condition. For a person with dementia, it is important to have these conversations early and as often as possible, while the individual can make decisions for themselves. The regionally developed resources from ‘My future wishes: Advance Care Planning for people with dementia in all care settings’ will support these conversations and should be widely used whether the person is in the community or in a care setting.
Kirklees Council continues to grant fund part of a role of a specialist end of life Admiral Nurse at The Kirkwood.
Which groups are most affected by this issue?
There are variances between men and women. The most robust way of looking at this is by understanding how many cases of dementia there are in every 1000 people in the population (Table 2).
In Kirklees:
- Prevalence of dementia increases with age for both genders.
- Women consistently show higher dementia prevalence than men in each age group.
- In the 85+ age group, dementia prevalence reaches:
- 160 per 1,000 women
- 120 per 1,000 men
Table 2 : Dementia prevalence per 1000 people in Kirklees, by age and gender
| Age Group | Male | Female |
| 65-69 | 8.2 | 9.5 |
| 70-74 | 14.5 | 17.8 |
| 75-79 | 28.3 | 35.6 |
| 80-84 | 65.7 | 78.2 |
| 85+ | 120.0 | 160.0 |
Source: NHS Primary Care Dementia Data, June 2025
This pattern reflects national trends, where dementia risk rises significantly with age and is more common among women, partly due to longer life expectancy.
Dementia is not restricted to age, gender or ethnicity and impacts individuals from all walks of life and communities. However, there are notable disparities in the risk, occurrence, diagnosis, and management of dementia. People with both dementia and depression have higher rates of disability and higher rates of hospital admission.
Some minority ethnic groups are more susceptible to conditions such as high blood pressure and diabetes, both of which are known to elevate dementia risk. Evidence suggests that these conditions may have a more pronounced impact on dementia risk in certain minoritised ethnic communities compared to White populations (Risk factors for dementia vary by ethnicity, study finds | ScienceDaily). For instance, high blood pressure is more likely to result in a stroke among Black individuals, and it is estimated that one in four people who experience a stroke will go on to develop dementia (Ethnicity and dementia risk – Alzheimer’s Research UK).
There is growing evidence to show dementia is more prevalent among Black African-Caribbean and South Asian populations compared to the White population in the UK, with these groups also experiencing an earlier onset of the condition. Additionally, these groups are more prone to high blood pressure, which is believed to increase the risk of vascular dementia, contributing to the higher prevalence. Locally, numbers of recorded diagnoses from these cohorts are historically very low, with low uptake of post diagnostic support services from people who do receive a diagnosis. Work will continue locally to ensure we raise awareness of dementia information, advice and support in these communities ensuring that public information materials are available in a range of community languages and accessible resource to support people to access pre and post diagnosis support. Use of the ADAPT toolkit will provide direction to better support the needs of these communities.
Living in areas of socioeconomic deprivation can significantly heighten dementia risk. As of 2020, South Asian and Black communities in the UK were among those most likely to reside in deprived neighbourhoods. These environments often come with limited access to quality food, education, healthcare, housing, and employment opportunities and tend to have higher levels of air pollution. Together, these factors contribute to a poorer quality of life and an elevated risk of developing dementia (Ethnicity and dementia risk – Alzheimer’s Research UK). While adopting healthier lifestyle habits can help reduce the risk of dementia, individuals living in deprived areas may face additional challenges in doing so. A lack of accessible support services and community resources can make it difficult for people to prioritise their health.
Where are they?
The prevalence of dementia by place in Kirklees is shown in Table 3. In summary:
- Holme Valley shows the highest estimated prevalence at 21.3 per 1,000.
- Huddersfield Central has the lowest at 17.8 per 1,000.
- Other areas such as the Colne Valley and Dewsbury also show relatively high rates.
These differences may reflect variations in age demographics, access to diagnostic services, reporting practices, population changes and data quality.
Table 3 : Estimated dementia prevalence per 1,000 people across different local areas in Kirklees
| Locality | Prevalence (per 1,000) |
| Holme Valley | 21.3 |
| Colne Valley | 20.7 |
| Dewsbury | 20.1 |
| Batley & Spen | 19.6 |
| Huddersfield North | 18.9 |
| Huddersfield South | 18.3 |
| Huddersfield Central | 17.8 |
Source: NHS Primary Care Dementia Data, June 2025
What are the assets around this issue?
We have recently reopened Knowl Park House Dementia Day Care Centre, which is a state of the art building designed in collaboration with the University of Stirling’s Dementia Services Development Centre. It provides a range of day opportunities for individuals living with dementia at its site in Mirfield. On the same site is the Kirklees Centre for Excellence building, which provides a mock showcase of room designs so that we directly show people living with dementia and their carers how important an enabling environment is for someone living with dementia. In addition, there are a number of key services delivering advice and information and showcasing small pieces of equipment, assistive technology and smart home devices, which may assist people to continue to live at home for longer (Knowl Park House – Day opportunities for adults with dementia | Kirklees Council).
The Live Life to the Full, Living with Dementia in Kirklees Guide is a snapshot of the offer of services to support people living with dementia and their carers in Kirklees. It is available online and in paper copy and in a number of community languages.
The Kirklees Dementia Empowerment and Engagement Project (DEEP) is the voice of people living with dementia in Kirklees. It is run by the Kirklees Dementia Hub is open to anyone with lived experience of dementia (Kirklees Dementia Engagement and Empowerment Project (DEEP)).
The Spotting the Signs of Dementia Leaflet assists people to initiate conversations around their cognition with their GP and was produced by the Kirklees DEEP group.
The Kirklees Dementia Friendly Design Tool, which can be used to apply to places and spaces in Kirklees to create more enabling environments for people living with dementia was produced in collaboration with University of Stirling’s Dementia Services Development Centre. This has been particularly useful for independent sector care homes to enable them to make subtle environmental changes and we would encourage any new care home or supported living provision to use the free design tool.
The Admiral Nurse Team at South West Yorkshire Partnership Foundation Trust are registered community mental health nurses who specialise in dementia care. They work collaboratively to offer person-centred support to carers and families of individuals living with dementia. Additionally, they partner with other agencies and care providers to deliver essential support, education, and information (Admiral nurses – South West Yorkshire Partnership NHS Foundation Trust).
The council has commissioned The Kirklees Dementia Hub which is a joint venture between Inspire North and Age UK to deliver the Kirklees Dementia Information Service to provide comprehensive information about services available within Kirklees and appropriate signposting support to individuals living with dementia and their carers to facilitate easier and earlier access to a full range of generic and specialist services. In addition, there are a small number of local dementia support groups and services available in both North and South Kirklees from befriending and dancing to lunch clubs and exercise classes. In addition, we continue to increase the number of dementia friends across the district to aspire to create Kirklees to be dementia friendly.
In addition, the Kirklees Working Together Better Partnership consists of 7 organisations commissioned by Kirklees Council to provide mental health support for individuals across Kirklees using a collaborative approach. The partnership’s goals include improving community mental health services, which are inclusive of individuals living with dementia, ensuring accessibility for all, increasing positive outcomes for service users, and fostering independence and resilience. The partnership includes Inspire North, Hoot Creative Arts, Cloverleaf Advocacy Services, Support to Recovery – The Great Outdoors, Cloverleaf Carer’s Count, Womens Centre and Waythrough Employment Services.
Views of local people
“J said he had learned more about dementia in the session than he had in his whole life, and I would agree. You are obviously very knowledgeable in this area which came through strongly. I know some colleagues who work in communities will be reaching out to you for additional sessions with community groups etc. I will certainly be sharing what I have learned with wider work colleagues and family.”
“I enjoy coming to the Church fellowship to be in company with friends. I have dementia but enjoy being with people.”
“Knowing we can come back into service on our dementia journey is comforting.”
“Easy to arrange an appointment. Very understanding and compassionate manner that instantly put me at ease. Offered lots of support options.”
“Empathy; Understanding; Sympathetic; Genuine; Caring; Approachable.”
“Online services are not suitable for me.”
What could commissioners and service planners consider?
- Raising public awareness about dementia, reducing the stigma and fear associated with dementia, raising awareness of the modifiable risk factors and encouraging people to seek help and obtain a diagnosis.
- Focusing on prevention and encouraging or enabling people to behave in ways which will improve their health outcomes (for example, relating to heart disease and stroke which increase the risk of vascular dementia) to reduce those risk factors associated with some dementias which we can do something about, e.g. alcohol use.
- Conduct focused efforts to reduce alcohol abuse in order to prevent or reduce alcohol-related dementias such as Korsokoff Syndrome.
- Focus on improving the diagnosis of dementia, as early as possible.
- Provide improved support for carers.
- More support for people to remain safely at home.
- Good quality and availability of residential and nursing care home places as well as day care and respite care.
- Increasing the range of accommodation choices for people with dementia, including extra care schemes.
- Influencing the design of accommodation to create environments which provide stimulation, enjoyment and dignified person-centred care.
- Improve the provision of intermediate care and rehabilitation for people living with dementia to reduce unnecessary or prolonged hospitalisation.
- Discussions around end of life should become part of normal conversation. There are taboos that need to be addressed if people with dementia are to have their end of life wishes acknowledged and acted upon.
- Continue to provide the Live Life to the Full, Living with Dementia in Kirklees guide which outlines the local dementia offer in Kirklees in a range of community languages in print and online.
- Support the implementation of dementia-friendly environments using the Kirklees Dementia Design Tool across a range of places and spaces in Kirklees.
- Promote assistive technology and equipment solutions so that people can remain independent for as long as possible in their own homes.
- Promote high quality support from a workforce trained to at least Tier 2 of the Dementia Training Standards Framework will become an increasing focus. This should include the importance of life story work (see ‘My life story’ template).
References and additional resources/links
Diagnosis of dementia – Dementia Statistics Hub (ARUK).
Dementia information – Alzheimer’s Research UK
https://dementiastatistics.org/about-dementia/deaths/
Dementia in Down’s syndrome – Alzheimer’s Research UK.
Kirklees Council: Reducing Your Risk Of Developing Dementia Leaflet
Kirklees Council: Live Life to the Full, Living with Dementia in Kirklees Guide,
Kirklees Council: Kirklees Dementia Friendly Design Tool
Kirklees Council Dementia Day Care, Knowl Park House – Day opportunities for adults with dementia | Kirklees Council
Kirklees Dementia Hub, Spotting the Signs of Dementia leaflet
Projecting Older People Population Information (POPPI)]. Available from: http://www.poppi.org.uk/
King’s Fund: Ethnic health inequalities and the NHS
Ethnicity and dementia risk – Alzheimer’s Research UK
Risk factors for dementia vary by ethnicity, study finds | ScienceDaily
Palliative and end of life care profile December 2023 update: Statistical commentary – GOV.UK
(ONS data)
Statistical commentary: dementia profile, December 2024 update – GOV.UK
Death registration summary statistics, England and Wales – Office for National Statistics
Marie Curie Public attitudes to death, dying and bereavement in the UK re-visited: 2023 survey
Deaths due to dementia – Dementia Statistics Hub
State of Caring 2022 report | Carers UK
Dementia Training Standards Framework | NHS England | Workforce, training and education
Admiral nurses – South West Yorkshire Partnership NHS Foundation Trust
My Future Wishes: Advance Care Planning For People With Dementia
Projecting Older People Population Information System
Projecting Adult Needs and Service Information System
Young onset dementia facts and figures – Young Dementia Network
Dementia UK My Life Story Template
See also: KJSA sections on Ageing Well and Mental Wellbeing
Date updated (and lead author initials): 22/07/25 (TS)